Managing Agenesis: From Orthodontics to Restorative Care
- Mar 18
- 3 min read
Updated: Mar 30
Where Growth, Timing, and Multidisciplinary Planning Converge
Managing agenesis is never a single‑phase problem—it’s a long arc that begins in mixed dentition and extends into early adulthood. For many young patients, the gaps go unnoticed until the teen years, when confidence, esthetics, and function all start to matter in new ways. This case follows Carson, a patient I first met in middle school, as she navigated years of orthodontics, transitional bonding, bone limitations, and restorative planning on her way to a complete smile.

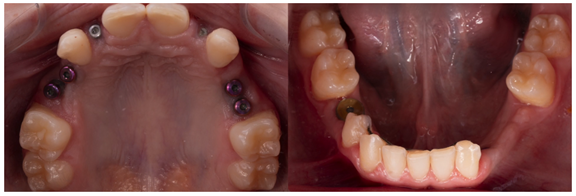
Carson was congenitally missing more than eight teeth, several of which were ankylosed primary teeth. Early coordination with the orthodontic and surgical teams focused on removing ankylosed teeth before they caused bone defects, monitoring growth, and determining the right moment for implant placement. Along the way, newer research emerged linking multiple‑tooth agenesis with elevated risks for certain cancers, including ovarian and colorectal cancer—an important consideration for recommending genetic testing in similar cases today.

Using Transitional Bonding to Guide Orthodontic Movement
When Carson first came to me, her centrals were undersized and spaced, her arch was severely underdeveloped, and her upper lip was extremely short and tight—a combination that complicated both esthetics and biomechanics.
We began by restoring the centrals with composite to ideal width and performing a minor gingivectomy.
Shade selection relied on:
Multi‑tab value‑based shade photos
Composite try‑ins
Polarized photography to eliminate reflections and narrow the shade family
As orthodontics progressed, space management became nearly impossible to evaluate visually because so many teeth were missing. To solve this, I had the orthodontist remove brackets from the canines so I could bond them to ideal width‑length proportions—not correcting axial inclination, simply establishing anatomical benchmarks. With idealized canines in place, the orthodontist could reposition brackets accurately and move teeth with far greater precision.
Planning Around Bone Limitations and Facial Support
By the time Carson completed orthodontics, her maxillary arch remained significantly retruded. Given her tight upper lip, mid‑face deficiency, and long treatment history, jaw surgery was something her family preferred to defer. The goal was to give her a full, confident smile in time for college.
Her implant sites offered limited bone, and implant positions were determined by what anatomy allowed rather than ideal locations.
Using digital design, we evaluated:
Emergence profiles
Restorative space
Potential need for splinting
Functional pathways
This step eliminated guesswork and ensured that on the day of restoration, we weren’t making “game‑day decisions.”
Provisionals That Transformed More Than Her Smile
Seeing Carson in full provisional restorations for the first time was emotional for everyone involved. After years of brackets, ankylosed teeth, missing teeth, and removable appliances she had to take out to eat, this was her first experience having a full set of teeth.

Bringing the facial surfaces forward also improved her lip support, softening the tight upper lip and balancing her facial profile. We kept the provisional shade she loved and planned intensive whitening for the lower teeth to harmonize the final result.
Delivering the Final Restorations
Seat day presented its own challenges. Her short vestibule and tight upper lip made isolation extremely difficult—even with a split dam. Using seating indices helped orient implant abutments accurately, and a 360‑style dam frame provided the added retraction needed since traditional U‑shaped frames offered little support superiorly.


Despite the complexity, the final restorations seated beautifully. Within a week or two, her tissue healed, the contours stabilized, and the transformation—functionally and esthetically—was remarkable.
Carson went off to college with a complete smile for the first time in her life. Few cases are as technically demanding, and few are as rewarding.

Three Key Takeaways from This Case:
Think long‑term from the start. Planning agenesis cases requires coordinating ortho, surgery, and restorative decisions through growth and into adulthood.
Use transitional bonding strategically. Idealized tooth forms give both the clinician and the orthodontist the anatomical blueprint needed for accurate space management.
Leverage digital design and lab communication. When anatomy limits implant positioning, digital workflows and ongoing collaboration with the technician eliminate surprises and improve outcomes.
If you want to see the full workflow and every step of Carson’s treatment journey, watch the complete clinical video: Managing Agenesis: From Orthodontics to Restorative Care.

Members:
Not a member?
The Case Continuum gives you access to ongoing case discussions and focused clinical lessons that show how decisions are made—step by step.
Plan with clarity, execute with confidence, and deliver predictable results. I’m not only teaching techniques—I’m showing you exactly how to think through clinical challenges, month after month.


